-
Email info@annpnc.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Surgery and Specialties, Faculty of Medicine and Pharmaceutical Sciences, University of Douala, Cameroon.
2Department of Internal Medicine and Pediatric, University School of Medicine, Wayne State, USA.
3Pediatric Surgery Unit, Laquintinie Hospital of Douala, Cameroon.
*Corresponding author: Pauline Mantho Fopa
Department of Surgery and Specialties, Faculty of
Medicine and Pharmaceutical Sciences, University of Douala, Cameroon.
Email ID: asandio@wayne.edu; mapaulefr2002@yahoo.fr
Received: Mar 16, 2026
Accepted: Apr 07, 2026
Published Online: Apr 14, 2026
Journal: Annals of Pediatrics and Neonatal Care
Copyright: Fopa PM et al. © All rights are reserved
Citation: Fopa PM, Bitchocka E, Tynes L, Tynes D, Ngowe MN. Anal prolapse in a child revealing a rectal adenoma: A case report. Ann Pediatr Neonatal Care. 2026; 2(1): 1014.
Rectal polyps are a common cause of rectal bleeding in children. In adolescents, their clinical presentation may be atypical and may reveal adenomatous lesions with potential for progression.
Case presentation: We report the case of a 14-year-old boy with no history of rectal prolapse during childhood who presented with rectal bleeding evolving for three months, associated with intermittent protrusion of a fleshy mass during defecation. After several consultations in peripheral healthcare facilities, he was referred for pediatric surgical evaluation. Clinical examination revealed a mass palpable in the rectal ampulla. Colonoscopy showed a large rectal polyp. Initial biopsy suggested an inflammatory polyp. Complete surgical excision was performed. Final histopathological examination revealed a tubular adenoma with low-grade dysplasia, without evidence of malignancy. The postoperative course was uneventful, and follow-up colonoscopy at two months was normal.
Conclusion: In adolescents, prolapse of an anal mass should raise suspicion of a rectal polyp. Colonoscopy with complete excision and histological examination is essential to establish the definitive diagnosis and ensure appropriate follow-up.
Keywords: Rectal polyp; Adolescent; Anal prolapse; Tubular adenoma; Colonoscopy.
Colorectal polyps represent a common cause of rectal bleeding in children and adolescents, accounting for up to 1-2% of pediatric endoscopic investigations [1,2]. In young children, these are most commonly juvenile hamartomatous polyps, which are benign and isolated, preferentially located in the rectosigmoid region [3]. However, in adolescents, the discovery of a symptomatic polyp should raise suspicion for more advanced histological lesions, particularly adenomatous polyps, which carry a potential for malignant transformation [4,5]. Prolapse of a rectal polyp may mimic true rectal prolapse, sometimes delaying diagnosis and appropriate management [6]. This case was observed in the Pediatric Surgery Department of Laquintinie Hospital in Douala, a tertiary referral center in Cameroon. We report the case of a 14-year-old adolescent in whom a prolapse resembling rectal prolapse revealed a tubular adenoma with low-grade dysplasia, highlighting the importance of complete endoscopic evaluation and systematic histological examination in this age group.
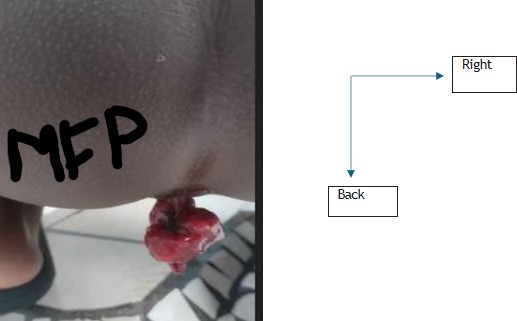
We report a clinical case managed in the Pediatric Surgery Department of Laquintinie Hospital in Douala, involving a 14-year-old adolescent admitted for rectal bleeding associated with anal exteriorization. The patient was a schoolboy with no notable medical history, particularly no history of rectal prolapse during early childhood. He initially consulted in May 2025 for anal bleeding evolving for three months, associated with intermittent protrusion of a fleshy mass through the anus during defecation, which reduced spontaneously after straining. The patient had been seen several times in peripheral health centers where he received symptomatic treatment without lasting improvement. Due to persistent symptoms, he was referred to our institution for pediatric surgical evaluation, where he was admitted on November 11, 2025. Clinical examination revealed a preserved general condition, a normal hemodynamic parameters, an unremarkable abdominal examination. Inspection of the anal margin was normal outside defecation episodes. Digital rectal examination revealed a palpable intrarectal mass in the rectal ampulla, soft in consistency and painless.
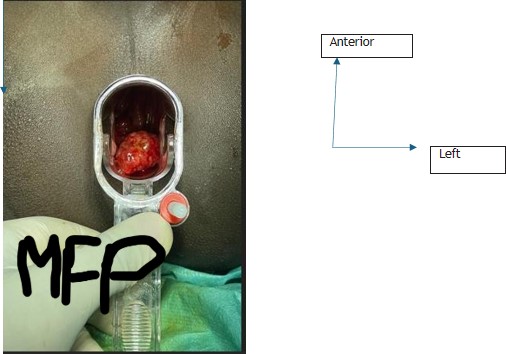
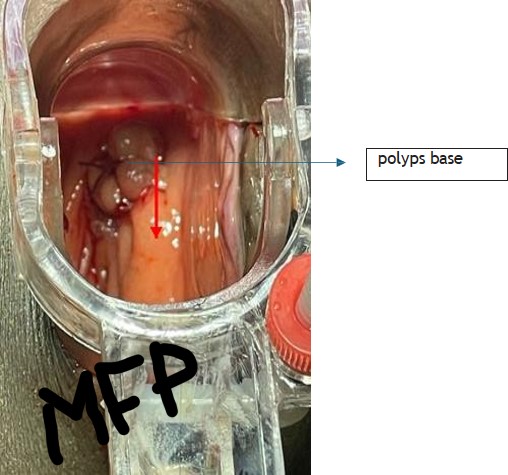
A total colonoscopy was indicated. It revealed a large pedunculated rectal polyp located in the distal rectum. A biopsy sample was obtained. Initial histopathological examination concluded inflammatory rectal polyp. Given the clinical symptoms (chronic bleeding and repeated prolapse) and the size of the lesion, surgical complete excision was indicated.
The patient underwent complete excision of the polyp, performed without intraoperative complications. The surgical specimen was sent for comprehensive histopathological analysis. Definitive histological analysis revealed a tubular adenoma of the rectum with low-grade dysplasia, without signs of malignancy.
Postoperative recovery was uncomplicated. At two months follow-up, the patient was asymptomatic, without recurrence of rectal bleeding, without anal protrusion. A follow-up colonoscopy performed during surveillance showed no abnormalities, confirming complete excision of the lesion. Endoscopic images, operative photographs, and pathology reports are available.
Clinical manifestations of rectal polyps in children typically include a painless rectal bleeding, a mucous discharge and more rarely an anal prolapse [1,3]. Prolapse is favored by a distal localization, a pedunculated morphology and a repeated straining during defecation [6]. Unlike juvenile polyps, which predominate before the age of 10 years, adenomatous polyps are more frequently diagnosed in adolescents, with an estimated prevalence of 3-10% of pediatric colorectal polyps [4,7]. These lesions are considered precursors of colorectal cancer, although malignant transformation remains rare in pediatric patients [5,8]. In our case, the initial biopsy suggested an inflammatory polyp, whereas the definitive histological examination of the surgical specimen revealed a tubular adenoma with low-grade dysplasia. This discrepancy is well described in the literature and highlights the limitations of partial biopsies, supporting the need for complete excision of symptomatic polypoid lesions [9].
Total colonoscopy is recommended in adolescents, even when a distal rectal polyp is identified, in order to search for synchronous lesions, to rule out a polyposis syndrome [2,7].
Endoscopic surveillance after adenoma removal is also recommended due to the risk of recurrence or metachronous lesions [5,8]. The favorable outcome observed in our patient, with normal follow-up colonoscopy at two months, is consistent with the literature when complete excision is achieved and no syndromic factors are identified [4,10].
In many African settings, rectal bleeding associated with anal exteriorization in adolescents is frequently interpreted as hemorrhoids or true rectal prolapse, leading to diagnostic delay and inappropriate management.
Limited access to pediatric colonoscopy and specialized care in sub-Saharan Africa contributes to underdiagnosis of rectal polyps, particularly adenomatous lesions in adolescents [5,11]. This observation highlights that symptomatic rectal polyps in African adolescents are not always benign juvenile polyps and may correspond to adenomas even in the absence of family history [12]. In these resource-limited settings, complete excision combined with histopathological examination is essential, since biopsy alone may be insufficient to establish a definitive diagnosis [5,12].
In adolescents, prolapse of an anal mass should raise suspicion of a rectal polyp until proven otherwise. Colonoscopy with complete excision and histological analysis is essential to establish the definitive diagnosis and guide follow-up. Although rare, adenomatous polyps must be actively investigated in this age group because of their potential for progression.