-
Email info@annpnc.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Dental Clinical Specialties, Faculty of Dentistry, Complutense University of Madrid, Spain.
2Madrid Health Service (SERMAS), Spain.
#Equal Contribution.
*Corresponding author: Antonia María Caleya-Zambrano
Department of Dental Clinical Specialties, Faculty of
Dentistry, Ramón y Cajal, s/n, Complutense University of Madrid, 28040 Madrid, Spain.
Received: May 05, 2025
Accepted: Jun 04, 2025
Published Online: Jun 11, 2025
Journal: Annals of Pediatrics and Neonatal Care
Copyright: Caleya-Zambrano AM et al. © All rights are reserved
Citation: Caleya-Zambrano AM, Gallardo-Lopez NE. Smile analysis and its relationship to anterior overjet in children and adolescents. Ann Pediatr Neonatal Care. 2025; 1(1): 1010.
Background: To analyze the relationship of the overjet and the smile characteristics on a sample of male and female Spanish children and adolescents.
Methods: A retrospective cross-sectional study was carried out on a sample of 44 photographs classified into two groups according to overjet (Group I: 0-5 mm, Group II: >5 mm). Parameters related to dentolabial relationship, amplitude, and smile symmetry were traced and evaluated applying a variance and covariance analysis as well as a correlation coefficient test.
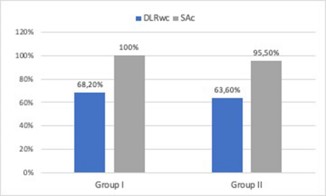
Results: No significant differences were observed regarding smile amplitude parameters. A predominance of non-contact dentolabial relationship was observed (group I: 68.20% and group II: 63.60%), as well as consonant smile arch (group I: 100%, group II: 95.50%). The ratio of the right oral corridor showed a proportional increase to the age increase of the subjects (r=0.392).
Conclusions: There were no significant differences on the smile characteristics of the sample related to overjet and sex, although the number of visible teeth and the ratio of the right buccal corridor showed a directly proportional relationship to the age increase regardless the overjet.
Keywords: Smile; Overjet; Children.
Abrevations: BCR: Buccal Corridor Radio; DLR: Dentolabial Relationship; Drlwc: Dentolabial Relationship Without Contact; Ohrqol: Oral Health-Related Quality of Life; SA: Smile Arch; Sac: Consonant Smile Arc. SDM: Superior Dental Midline; ULH: Upper Lip Height; SI: Smile Index; VT: Number of Visible Teeth; Vts: Superior Visible Teeth.
The Oral Health-Related Quality of Life (OHRQoL) of an individual can be influenced by four main aspects: function (eating, chewing, speaking), pain or discomfort, psychological factors and social well-being [1-3]. The smile is a facial expression that may reveal important aspects of the OHRQoL. Psychological aspects, such as the perception of the subject of his own smile or social aspects, such as others perception of the subject’s smile may be reflected in smile patterns such as amplitude of the smile and number of teeth that are shown, as well as the relaxation shown when smiling [4].
From a child’s psychological point of view, a smile can also reflect aspects such as interpersonal relationships, as well as self-esteem. Patel et al. [5] observed that children who did not have cavities had a more positive perception of their smile and showed a greater number of teeth when they smiled. Another study conducted by Golai et al. [4] determined that dental trauma produces a negative impact on smile patterns, confidence, and social interactions in children.
Malocclusions are a group of oral pathologies that lead to aesthetic problems in a greater or lesser degree. It has been described that maxillary and mandibular protrusion, deviation of the midline, diastemas, open bite, and maxillary irregularity are, in this order, directly associated with the presence of negative impacts on the quality of life [6]. Therefore, we hypothesized that a relationship between overjet variations and smile characteristics may be observed. The studies that analyze the relationship of the malocclusions and the characteristics of the smile in children and adolescents are scarce, in addition they usually only analyze the number of exposed teeth and the amplitude of the smile. For all the above mentioned, this study aims to analyze the relationship of the overjet and the smile characteristics in a sample of Spanish children and adolescents.
A cross-sectional retrospective study was carried out. The orthodontic study was done for diagnostic purpose, not for this study. Ethical review and approval were waived for this study due to that the orthodontic study are records that were requested out for diagnose purpose unrelated to this study in a justified manner and with the consent of the patient and/or legal guardians, being stored in the databases of private Dental Clinic. The retrospective nature of the study, compiling demographic and radiographic data in accordance with current Data Protection regulations, makes the report of the Ethics Committee unnecessary. Written informed consent has been obtained from all participants to publish this paper.
Frontal photographs, taken with a Nikon D2X camera, 105 mm Nikon lens, macro f 2.8, Nikon Sb 600 flash, of children and adolescents who attended a private practice in Madrid, were used. An informed permission was signed by the parents of all participants, permitting the use of their clinical data for research purposes.
A sample size calculation was made, based on a similar study [7] and a minimum of 12 individuals were necessary on each group, however, due to the availability of a higher number of photos an n=22 per group was established. Using a sampling technique of consecutive cases, photographs of Spanish subjects, of maximum 16 years old, with permanent dentition or second phase mixed dentition, with complete eruption of both maxillary canines and, without previous orthodontic treatment or any systemic disease, congenital orofacial malformation or neuromuscular involvement were selected. Photographs in which the subject presented absence of a tooth in the anterior sector or with presence of dental alterations of shape, structure or color and, bad quality or incomplete photographs were excluded.
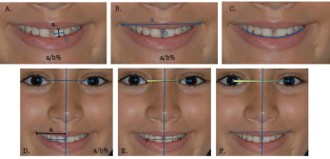
Two groups were established according to overjet (Group I: 0-5 mm, Group II: >5 mm), which was documented in the clinical records that were accessed. Nine parameters were recorded as described in Table 1 and some of them are shown in Figure 1. Prior tracing these parameters, the bipupilar line and the midline were drawn as reference lines. The linear measurement digitization tool was used in Adobe Photoshop (CS, Adobe Systems, Inc., San Jose, CA, USA) taking the pixel as unit of measurement. All measurements were made by a single researcher previously calibrated and were repeated on a different session in ten randomly chosen photographs.
The statistical analysis was carried out using the SPSS 25.0 program for Windows (SPSS Inc., Chicago, Ill., USA). The Exact Fisher test was used to compare the variables Dentolabial Relationship (DLR), Smile Arch (SA) and Superior Dental Midline (SDM). An ANCOVA was carried out and allowed the creation of a model with the factors: group, sex, group-sex, and the covariate age; as well as the correction of age in the variables: superior Visible Teeth (VTs) and right Buccal Corridor Radio (BCRr) to be compared according to sex and group using the MannWhitney U test. Pearson correlation coefficient was used to relate all the parameters with age; and ANOVA test was applied to compare the bilateral measurements. Finally, the Kappa index and the t-Student test were carried out to verify the measurements reliability.
Two hundred and nine photographic records were evaluated of which 44 met the selection criteria. Table 2 shows the distribution of the sample into two groups according to overjet, age and sex.
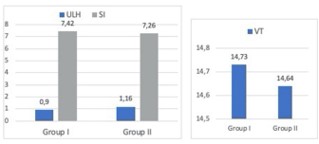
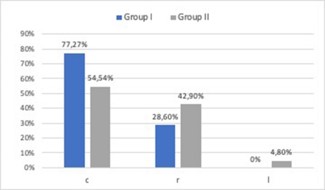
The parameters referring to the amplitude of the smile and the dentolabial relationship were similar in both groups, the differences observed were not statistically significant (Figure 2 & 3). The superior dental midline was coincident with the facial midline in most subjects of both groups (Figure 4); while, regarding the bilateral parameters, the group with the least overjet (Group I) showed slightly higher values (Table 3).
All these factors were compared considering group, sex and age. Statistically significant differences were observed between overjet values of Group I (3.594 mm) and II (6.536 mm). Regardless the group to which they belonged, statistically significant differences were observed between the variables: superior visible teeth and right buccal corridor radio when correlating them with the age of the subjects (Table 4); whilst left buccal corridor radio showed significant differences considering the position of the right or left superior dental midline (SDMr: 1.8346 px and SDMl: 1.6841 px). No significant differences were found (p=0.124) regarding to sex.
| Parameters | Criteria |
|---|---|
| Visible teeth | Number of partially or totally exposed teeth: • Superior teeth • Inferior teeth |
| Upper lip height | Incisolabial distance / Central superior incisor width |
| Smile index | Smile width / Interlabial distance |
| Smile arch | The curvature of the maxillary incisal edges and canines relative to the curvature of the lower lip on smile: • Consonant • Non-consonant: flat or inverted |
| Dentolabial relationship | • Relation of the lower lip vermilion border with any point of one of the CSI incisal edge: • Without contact • With contact • With interposition • Covered: superimposition of the lower lip vermilion border on the incisal edge of any of the central superior incisor |
| Superior dental midline | • Coincident with the facial midline • Not coincident: Deflected or tilted to the right or to the left |
| Buccal corridor ratio | Horizontal distance from the apex of the outer commissure to right or left / horizontal distance from the cusp of the canine to the facial midline: right or left |
| Commissural elevation | Angle formed when perpendicularly moving the intercommissural line to a point where it intersects the bipupilar line |
| Occlusal frontal plane | Angle formed when perpendicularly moving the canine intercuspal line to a point it intersects the bipupilar line |
| Group | Sex | Age | n | ||
| Female (%) | Male (%) | media | Standard Deviation | ||
|---|---|---|---|---|---|
| Group I | 16 (72,7) | 6 (27,3) | 12,64 | 1,53 | 22 |
| Group II | 10 (45,5) | 12 (54,5) | 12,73 | 1,55 | 22 |
| Total | 26 (59,1) | 18 (40,9) | 12,69 | 1,52 | 44 |
| Group I | Group II | |||||
| n | media | Standard Deviation | n | media | Standard Deviation | |
|---|---|---|---|---|---|---|
| Left buccal corridor ratio | 20 | 1,73 | 0,15 | 20 | 1,75 | 0,18 |
| Right buccal corridor ratio | 20 | 1,66 | 0,17 | 20 | 1,72 | 0,10 |
| Left commissural elevation | 15 | 0,91 | 0,96 | 15 | 0,89 | 0,72 |
| Right commissural elevation | 9 | 1,14 | 2,16 | 10 | 0,97 | 0,87 |
| Left occlusal frontal plane | 11 | 2,06 | 1,4 | 13 | 1,95 | 1,77 |
| Right occlusal frontal plane | 8 | 2,45 | 2,24 | 8 | 1,09 | 0,91 |
| n | Pearson correlation | p-value | |
|---|---|---|---|
| Overjet | 44 | - 0,183 | 0,234 |
| Superior visible teeth | 44 | 0,328* | 0,030 |
| Inferior visible teeth | 44 | 0,205 | 0,182 |
| Visible teeth | 44 | 0,281 | 0,064 |
| Upper lip height | 43 | - 0,146 | 0,352 |
| Smile index | 43 | - 0,048 | 0,759 |
| Left buccal corridor ratio | 40 | 0,231 | 0,151 |
| Right buccal corridor ratio | 40 | 0,392* | 0,012 |
| Left commissural elevation | 30 | 0,122 | 0,519 |
| Right commissural elevation | 19 | 0,037 | 0,880 |
| Left occlusal frontal plane | 24 | 0,036 | 0,867 |
| Right occlusal frontal plane | 16 | 0,324 | 0,221 |
*p<0,05
A systematic review of 2014 [8] showed that between 43% and 78% of the studied population had some type of malocclusion, while research carried out in Europe has recorded a ratio of 1:5 or 1:6 school children in need of Orthodontic treatment [9]. Moreover, it is precisely in this period that malocclusion treatments are commonly initiated; thus, our study focused on a population that oscillated between nine and 16 years old.
Photographic recording was used to study the smile given its characteristics of consistency and reproducibility [7,10-12]. Although there are variations throughout the literature regarding the type of registration preferred, it has been described that there is no clinically significant difference between the images of smiles of subjects captured by clinical photography and the smiles of the same subjects obtained from digital video clips [13].
The measurement of the parameters was recorded in pixels, which allowed eliminating possible conversion errors to other measurements. These parameters were recorded as proportions, since it has been described that these are of greater value than the linear measurements [14]; and as angular measurements, which allowed to objectively measure asymmetries in the participants’ smile.
The parameters related to the amplitude of the smile did not show significant differences when comparing them according to the group or sex, which agrees with the results of Mcnamara et al. [14] and Shah et al. [1] In addition, a directly proportional relationship was observed between the variable VTs with the age of the subjects, which differs from the results reported by Cheng et al. [7]. We believe that part of the explanation for this phenomenon is the age of the subjects, due to the fact that Cheng et al. [7] study sample was formed by adults. However, our results do not correspond with the ones of Golai et al. [4] or Patel et al. [5] who observed a decrease of visible teeth number in presence of the pathology studied (trauma and dental caries respectively) which may be explained by the clinical characteristics of an increased overjet, which leads to greater dental exposure.
Regarding the smile arch, some studies [11] have observed a loss of the maxillary incisors curve in relation to the lower lip curve in patients who had received orthodontic treatment. In agreement with this, in our study we observed a predominance of a consonant smile arch since the patients in our sample had not received any orthodontic treatment.
Although the correlation observed between BCRr and age is low (r=0.392), it is a result that contradicts those exposed in two other studies that were carried out in adult patients. Whilst, Yang et al. [12] suggested that there is a certain relationship between the dental prominence in adults and the buccal corridors, since they observed that the more anterior and downward the upper incisors are, and the lower and anterior the lower incisors are, the smaller the area of the buccal corridor is. Finally, the relationship of the BCRl with the SDM, became difficult to interpret because only one subject presented deviation from the latter to the left side, which made it impossible to perform post-hoc statistical tests. When observing the data, it is logical to think that the buccal corridors increase as the middle line deviates towards the opposite side, however, this affirmation must be verified in future studies.
It is necessary to perform new studies on smile analysis in pediatric population, taking into account other factors such as occlusal and psychological aspects, in order to relate them to the OHQolr. There are studies that analyse the quality of life related to oral health and malocclusions, such as the one by Elyaskhil et al, which analyses how the severity of a malocclusion can affect the QHRQolr, with the psychological domain being the most affected and in the female gender [15]. Other research confirms that agenesis of lateral incisors can have a negative impact on OHQolr and that closing spaces with orthodontic treatment has a positive impact on quality of life [16]. Furthermore, treatment of malocclusions such as open bite improves OHQol [17], although systematic reviews have found this association to be modest [18]. However, there is evidence that poor oral health does have a negative impact on OHRQoL [19].
Based on this study’s results, the following conclusions can be made:
1. Spanish children and adolescents who were part of the sample did not show different smile characteristics in presence of a greater or lesser anterior overjet.
2. The number of visible teeth and the ratio of the right buccal corridor showed a directly proportional relationship to age increase, regardless the overjet.
3. The authors believe that future studies on how smile characteristics influence the OHRQoL.
Ethics approval and consent to participate: The records were made for the purpose of initiating orthodontic treatment at the practice because all individuals had tome type of malocclusion. The parent/legal guardian of the patients signed a written consent for the use of records for purposes investigations.
Acknowledgements: We are grateful for the patients and their legal guardians for their participation in this study and their contribution to science. As well as the University Complutense of Madrid and Madrid Health Service for promoting research and always giving us their unconditional support.
Author’s contributions: Authors’ contributions A.C-Z. contributed to investigation, resources, data curation, writing review and editing. A.D-S. contributed to conceptualization, methodology, formal analysis, data curation, investigation, writing-original draft. NG-L. conceptualization, investigation, resources, validation, writing-review and editing, supervision. All authors read and approved the final manuscript.
Funding: This project has not obtained any funding
Consent for publication: I am the author responsible for the submission of this article and I accept the conditions of submission and the BMC Copyright and License Agreement as detailed above.
Competing interests: No, I declare that the authors have no competing interests as defined by BMC, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Availability of data and materials: All of the material is owned by the authors and/or no permissions are required. The datasets generated during and analysed during the current study are not publicly available due to [national data protection law] but are available from the corresponding author on reasonable request.