-
Email info@annpnc.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi, India.
*Corresponding author: Prabudh Goel
Professor of Paediatric Surgery, All India Institute of
Medical Sciences, New Delhi, India.
Email ID: drprabudhgoel@gmail.com
Tel: +91-9999944511
Received: Apr 08, 2025
Accepted: May 18, 2025
Published Online: May 25, 2025
Journal: Annals of Pediatrics and Neonatal Care
Copyright: Agarwal S et al. © All rights are reserved
Citation: Phugar S, Goel P. The language of the neonates: Understanding and responding to nonverbal communication in neonatal care. Ann Pediatr Neonatal Care. 2025; 1(1): 1009.
Neonates, despite their inability to verbalize, possess sophisticated communication systems that convey their physiological and emotional states through behavioral and autonomic signals. Effective communication with neonates represents a critical skill for healthcare professionals in neonatal care settings. Unlike verbal communication with older patients, neonatal communication relies on interpreting subtle behavioral, physiological, and autonomic signals. This review examines the current evidence on neonatal communication patterns, assessment tools, and clinical applications. Special emphasis is placed on the role of observational assessment and parental involvement in understanding neonatal cues. Evidence suggests that structured observation protocols and parent education significantly improve clinical outcomes and parentinfant bonding. Recommendations for clinical practice include integrated communication-based care models that recognize the neonate as an active communicator rather than a passive recipient of care. This paradigm shift towards communication-centered neonatal care has implications for pain management, developmental support, and early detection of pathological conditions.
The neonatal period is a crucial phase of rapid development and adjustment to life outside the womb, during which infants must develop effective ways to communicate their needs. Unlike older patients who can articulate their experiences, neonates depend solely on nonverbal behavioral and physiological cues to convey their states, needs, and reactions to their surroundings. This is particularly significant given that newborns experience pain more intensely and for a longer duration than adults [1]. Historically, neonates were viewed as having limited capacity for meaningful communication, but research over the past four decades has demonstrated sophisticated communication systems that, when properly interpreted, can guide clinical care [2-3].
The clinical significance of understanding neonatal communication extends beyond basic care to influence medical decision-making, pain management, neurodevelopmental support, and early detection of pathology. Samane et al (2022) [4] demonstrated that care protocols based on reading and responding to infant behavioral cues resulted in improved short and long-term outcomes for preterm infants, including reduced ventilation days, earlier oral feeding, and improved neurodevelopmental outcomes.
Clinical vignette: Nurse Sharma, with 15 years of NICU experience, noticed subtle changes in baby Riya’s facial expressions and limb movements during a routine assessment. Though vital signs remained stable, she recognized these as stress cues and adjusted her positioning. Within minutes, her oxygen saturation improved by 5%. When asked how she knew, she replied, “She was telling me she was uncomfortable—I just needed to listen”.
Neurological development and communication capacity
The neurological foundation for neonatal communication begins during fetal development but continues to evolve rapidly after birth. Many studies have documented that by 32 weeks gestation, the neural pathways necessary for processing sensory information and generating organized responses are established, though significant maturation continues throughout the first year of life [5-7]. This neurological architecture enables neonates to detect, process, and respond to environmental stimuli in increasingly organized ways.
Cortical and subcortical structures involved in communication include the limbic system (amygdala), autonomic nervous system, and cortical networks that modulate attention, arousal, and basic information processing (Figure 1).

Sensory systems as communication channels
Each sensory system contributes uniquely to neonatal communication:
Tactile system: The most developmentally mature sensory system at birth serves as a primary channel for both receiving and expressing communication. Ellingsen et al (2016) [8] found that carefully calibrated touch can elicit specific behavioral and cortical responses that indicate comfort or distress in newborns.
Auditory system: Functional from approximately 24 weeks gestation, allows neonates to recognize and respond differentially to familiar voices. A meta-analysis documented the beneficial effects of maternal voice simulation on heart rate stability and oxygen saturation [9] demonstrating not only recognition but communication of preference through behavioral state changes.
Visual system: Though immature at birth with acuity limited to approximately 30 cm, supports the development of face recognition and social engagement. Eye contact, gaze aversion, and visual tracking provide important communicative signals, particularly regarding attention capacity and social interest [10].
Olfactory system: Allows recognition of maternal scent and breast milk. Various studies have demonstrated that neonates communicate preference through orientating behaviors toward maternal scent within hours of birth [11-13].
Vocalization patterns
The neonatal cry represents the most obvious communication signal and has been extensively studied. Acoustic analysis has identified specific cry parameters that communicate distinct needs or conditions:
Basic cry parameters with communicative value:
• Fundamental frequency (pitch)
• Duration and rhythmicity
• Melodic contours
• Presence of dysphonation or hyperphonation
Several studies [14-17] have tried to analyse the different cries of newborns and found that specific cry characteristics correlated with particular conditions:
• Pain cries: characterized by higher pitch, longer duration, and shorter latency to peak intensity [16]
• Hunger cries: rhythmic pattern with moderate intensity [17-18]
• Fatigue cries: lower intensity with irregular patterns
Non-cry vocalizations (coos, grunts, sighs) also carry communicative intent, particularly regarding respiratory effort and comfort level [19].
Parent perspective: “I never knew babies had different cries until my daughter Shikha was born premature,” recalls Meera, mother of a 32-week preemie. “Within days, I could distinguish between her hungry cry—rhythmic and building in intensity— and her pain cry, which started suddenly and pierced my heart. Her medical team taught me that recognizing these differences wasn’t just intuitive; it was science.”
Body language and motor signals
Motor behavior comprises a rich communication system, with different movements and postures signaling distinct physiological and emotional states:
Posture and tone:
• Flexion: typically signals security and self-regulation
• Extension: may indicate distress, pain, or neurological issues
• Asymmetrical posturing: often signals discomfort or neurological dysfunction
Limb movements:
• Smooth, coordinated movements: typically indicate an organized state
• Frantic, disorganized movements: often signal distress
• Tremors: may indicate stress, withdrawal, or neurological issues
Prechtl (1990) [20] established that general movement assessment provides valuable information about neurological integrity and developmental trajectory, demonstrating how motor behavior serves both immediate communication and prognostic indicators.
Facial expressions
Facial expressions represent one of the most readable communication channels in neonates. Distinct facial configurations have been reliably associated with specific states:
Pain expressions such as brow bulge, eye squeeze, nasolabial furrow, open lips, stretched mouth and taut tongue form the basis of the Neonatal Facial Coding System (NFCS), which Grunau et al. (1987) [21] validated as a reliable measure of pain in both term and preterm infants.

| Communication Channel | Observable Signs | Potential Interpretation | Recommended Response |
|---|---|---|---|
| Vocalization | High-pitched, intense cry with short latency to peak | Pain or acute distress | Prompt assessment for source of pain; appropriate analgesia; containment support |
| Rhythmic, moderate intensity cry with building pattern | Hunger | Offer feeding; assess feeding readiness cues | |
| Low intensity cry with irregular patterns | Fatigue | Reduce stimulation; support sleep transitions; postpone non-urgent procedures | |
| Grunting, sighing | Respiratory effort; self-regulation attempt | Monitor respiratory status; support positioning | |
| Body Language | Flexed posture, hands to midline | Security; self-regulation | Maintain supportive positioning; positive reinforcement |
| Extended posture, arching | Distress; discomfort; neurological issue | Reduce stimuli; containment support; neurological assessment if persistent | |
| Smooth, coordinated movements | Organized state; neurological integrity | Continue current care approach; opportunity for engagement | |
| Frantic, disorganized movements | Overwhelming stress or stimuli | Reduce environmental stimuli; provide boundaries; containment holding | |
| Tremors | Stress; withdrawal; neurological concern | Medical evaluation; consider metabolic factors; swaddling support | |
| Facial Expressions | Brow bulge, eye squeeze, nasolabial furrow | Pain | Pain assessment; appropriate management; comfort measures |
| Bright eyes, smooth brow, focused gaze | Attention/interest; optimal interaction state | Opportunity for engagement; social interaction | |
| Relaxed face, subtle smile | Pleasure/contentment | Positive reinforcement; opportunity to strengthen bonding | |
| Glazed eyes, drooping eyelids | Fatigue/disengagement | End stimulation; support sleep transition | |
| Autonomic Indicators | Stable heart rate with normal variability | Physiological regulation; comfort | Continue current care approach |
| Tachycardia | Stress; pain; fever | Comprehensive assessment; reduce stressors; pain evaluation | |
| Bradycardia | Severe distress; vagal response; neurologi- cal issue | Immediate medical evaluation; support ventilation if needed | |
| Regular breathing | Physiological stability | Continue current care approach | |
| Irregular breathing; pauses | Stress; immature respiratory control | Positioning support; respiratory assessment; monitor closely | |
| Mottled skin | Temperature instability; stress response | Thermoregulation support; reduce environmental stressors | |
| Circumoral cyanosis | Respiratory compromise | Oxygen assessment; positioning; respiratory support as needed |
Note: This table provides general guidelines. Individual neonates may display unique communication patterns that become recognizable with consistent observation. Integration of multiple channels provides the most accurate interpretation
Autonomic and physiological indicators
Physiological parameters serve as a communication system that bypasses conscious control (Table 1).
Johnston et al (2019) demonstrated that subtle changes in heart rate variability often precede clinical deterioration by hours, highlighting how physiological communication can provide early warning signs before overt behavioral changes are visible [22].
Structured observation techniques
Systematic observation represents the cornerstone of interpreting neonatal communication. Several validated assessment tools formalize this process:
The neonatal behavioral assessment scale (NBAS): Developed by Brazelton and colleagues (1995) [23], the NBAS evaluates 28 behavioral items and 18 reflexes. The NBAS has demonstrated utility in identifying individual differences in communication styles and guiding personalized care approaches.
Assessment of preterm infant behavior (APIB): Als et al. (2012) [24] developed a specialized observational tool for preterm infants that examines interactions across the following subsystems: (i) Physiology, (ii) Motor, (iii) State, (iv) Attention/ Interaction, (v) Regulatory, and (vi) Examiner Facilitation.
The APIB enables clinicians to identify thresholds at which communication signals indicate stress versus stability, guiding appropriately timed interventions.
Technology-assisted observation
Emerging technologies enhance observational capacity:
Video analysis systems: The video recording of children with subsequent analysis improves detection of subtle communication signals often missed in real-time observation, particularly brief expressions of pain or stress that might occur [25].
Physiological monitoring integration: Lungu et al. (2024) [26] developed systems that integrate behavioral observations with physiological monitoring (heart rate, oxygen saturation, respiratory rate, skin temperature), creating multimodal communication profiles that improved detection of sepsis by 6-48 hours before clinical diagnosis.
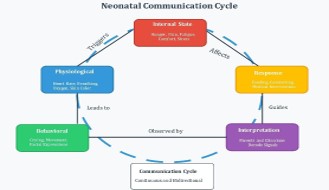
Parental attunement and responsiveness
Parents naturally develop specialized expertise in reading their infant’s unique communication patterns. This process of attunement begins prenatally and accelerates after birth. Feldman et al. (2014) documented that by two weeks postpartum, mothers could distinguish their infant’s cries from those of other neonates [27-28] as it evokes a unique pattern of neural responses [29], demonstrating rapid learning of individual communication signatures.
The parent-infant communication system operates bidirectionally (Figure 3).
Family journey: When twins Karan and Arjun were born at 34 weeks, their father felt overwhelmed by the NICU environment. “The monitors and alarms were my guide at first,” he explains. “But after participating in the parent communication workshop, I started noticing how Karan would bring his hand to his face when overstimulated, while Arjun would hiccup when he needed burping. Understanding these personal ‘languages’ transformed me from a visitor to their dad—someone who truly knew them.”
Supporting parents as primary interpreters
Evidence indicates that structured education enhances parental competence in interpreting neonatal signals. Two studies [4,30] have evaluated how teaching mothers to provide behavioral cue-based feeding and found to have several positive effects on the health of the infants’ including greater weight gain, head circumference and fewer oxygen desaturations.
Individualized developmental care
Newborn Individualized Developmental Care and Assessment Program (NIDCAP) [31] represents the most comprehensive application of communication-based care. This approach uses detailed behavioral observations to create individualized care plans responsive to each infant’s unique communication patterns.
Evidence for NIDCAP effectiveness: A systematic review by Wallin and Eriksson (2009) [32] examined the effects of the NI-DCAP based on six randomized controlled trials. The findings indicated several benefits, including enhanced psychomotor development, reduced duration of ventilation or CPAP support, shorter dependence on supplemental oxygen, and improved growth in weight and head circumference.
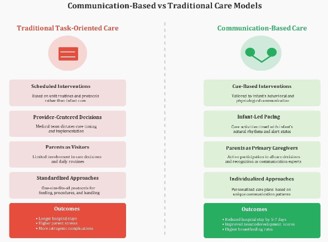
A communication-based model can guide clinical decisionmaking and improve outcomes (Figure 4).
Family-centered communication approaches
Family Integrated Care (FICare) models incorporate parents as primary caregivers who read and respond to infant cues with professional support. Studies [33-36] found that FICare implementation resulted in:
• Improved weight gain
• Reduced parental stress and anxiety
• Increased breastfeeding rates
• Higher parent satisfaction and confidence
• Earlier discharge
The success of these models demonstrates the clinical value of prioritizing the parent-infant communication system as a cornerstone of neonatal care.
Pain assessment and management
Pain assessment represents one of the most critical applications of neonatal communication interpretation. A systematic review in 2021 [37] identified 20 previously published pain scales while a previous systematic review had identified 65 scales related to assess pain and sedation levels in neonates out of which only 28 were tested for construct validity, internal consistency, and interrater reliability [38]. There are different scales available for pain assessment as Premature Infant Pain Profile Revised (PIPP-R) [39], COMFORT-B [40], Early Feeding Skills Assessment (EFS) [41] and many more as given in Table 2.
Interdisciplinary approach: During a heel stick procedure for baby Sonia, the coordinated care team demonstrated how neonatal communication guide practice. The phlebotomist paused when Sonia displayed disengagement cues (finger splaying, gaze aversion), allowing the nurse to provide containment holding and a pacifier. The procedure resumed only when Sonia displayed regulation cues. This responsive approach reduced the procedure time by 40% and minimized recovery time, as documented in her chart: “Communication-responsive care applied during an invasive procedure with a positive outcome.”
Units implementing feeding protocols based on these communication signals reported:
• Earlier transition to full oral feeding
• Fewer feeding-related adverse events
• Improved weight gain trajectories
• Higher parental confidence
| Assessment Tool | Developer & Year | Target Population | Key Components | Validation Status | Clinical Utility |
|---|---|---|---|---|---|
| Neonatal Behav- ioral Assessment Scale (NBAS) | Brazelton et al. [23] | Full-term and stable preterm infants | • 28 behavioral items • 18 reflexes • Stress responses |
Extensively validated across diverse populations and cultures | • Identification of individual communication styles • Guide for personalized care • Parent education tool • Prediction of developmental trajectories |
| Assessment of Preterm Infant Behavior (APIB) | Als et al. [24] | Preterm infants | • Physiological subsystem • Motor subsystem • State subsystem • Attention/ Interaction • Self-regulation • Examiner facilitation |
Validated in NICU populations; strong inter rater-reliability | • Identification of stress thresholds • Guide for NIDCAP interventions • Documentation of neurobehavioral organization • Measurement of intervention effectiveness |
| Neonatal Facial Coding System (NFCS) | Grunau & Craig [21] | Term and preterm infants | • Brow bulge • Eye squeeze • Nasolabial furrow • Open lips • Stretched mouth • Taut tongue • Lip pursuing • Chin Quiver |
Validated for pain assessment with high specificity | • Objective pain assessment • Research tool for procedural interventions • Training tool for clinicians • Documentation of pain response |
| Premature Infant Pain Profile Revised (PIPP-R) | Stevens et al. [39] | Preterm and term infants | • Contextual factors (gestational age, behavioral state) • Physiological indicators (heart rate, oxygen saturation) • Facial actions |
Validated with excellent psychometric properties across gestational ages | • Comprehensive pain assessment • Guide for analgesic interventions • Quality improvement metric • Research tool |
| COMFORT-B Scale | Dijk et al. [40] | NICU & PICU patients | • Alertness • Calmness/Agitation • Respiratory response • Physical movement • Blood pressure • Heart rate • Muscle tone • Facial tension |
Validated for pain and sedation assessment | • Sedation management • Post-operative pain assessment • Procedural distress monitoring • Ventilated infant assessment |
| Early Feeding Skills Assessment (EFS) | Thoyre et al. [41] | Infants upto 6 months | • Readiness cues • Respiratory regulation • Oral-Motor function • Swallowing coordination • Feeding engagement • Physiological stability |
• Recovery
Validated for preterm feeding assessment | • Feeding protocol development • Prevention of feeding complications • Parental education • Discharge readiness |
| Communication domain | Evidence-based recommendation | Practical application | Expected outcome |
|---|---|---|---|
| Environmental context | Minimize noxious stimuli during communication attempts | • Reduce ambient noise to <45dB • Dim lights during interactions • Cluster care activities • Create "quiet hours" |
• Improved signal clarity • Enhanced attention capacity • More organized behavioral responses • Reduced stress biomarkers |
| Timing & pacing | Match communication attempts to infant state and readiness | • Observe for "alert quiet" state before interaction • Respect sleep cycles • Allow 5-10 seconds for response • Monitor autonomic stability |
• Higher quality interactions • Reduced energy expenditure • Better self-regulation • Appropriate developmental stimulation |
| Multisensory approach | Layer communication channels strategically | • Begin with containment touch before visual stimulus • Add voice only after touch is well-tolerated • Introduce one sensory channel at a time • Observe for integration versus overload |
• Improved sensory processing • Enhanced self-regulation • Appropriate neurodevelopmental support • Prevention of sensory defensiveness |
| Contingent responsiveness | Respond promptly and appropriately to infant signals | • Acknowledge all communication attempts • Modify approach based on feedback • Document individual patterns • Share observations across care team |
• Reinforcement of communication efforts • Development of secure attachment • Enhanced brain connectivity • Reduced stress responses |
| Touch communication | Use calibrated touch as primary communication channel | • Begin with firm, still containing touch • Avoid light, ticklish touch • Use hand swaddling during procedures • Teach parents appropriate touch modalities |
• Improved physiological stability • Enhanced pain tolerance • Better sleep organization • Appropriate sensory development |
| Vocal communication | Optimize vocal characteristics when speaking to infants | • Use higher pitched, melodic speech • Speak at 15-30 cm distance • Allow longer pauses between phrases • Match tone to desired state (calming vs. alerting) |
• Enhanced auditory processing • Improved language outcomes • Stronger parent-infant bonding • Better state regulation |
| Parent professional partner- ship communication domain | Promote parents as primary communication interpreters | • Involve parents in rounds discussions • Document parent observations • Create communication journals • Validate parental interpretations |
• Increased parental confidence • Improved care continuity • Enhanced infant self-regulation • Earlier recognition of changes |
| Documentation | Systematically record communi- cation patterns | • Create standardized communication section in chart • Document both stress and engagement cues • Note changes over time • Include parent observations |
• Individualized care planning • Earlier detection of pathology • Improved handoff quality • Enhanced continuity of care |
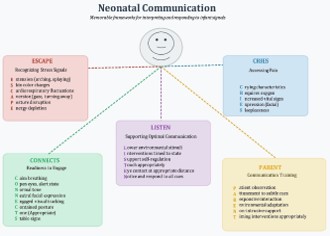
Guidelines for communicating with neonates
Table 3 provides guidelines for healthcare professionals and parents to optimize communication with neonates.
Despite significant advances in understanding neonatal communication, important knowledge gaps remain:
Biomarker correlation: Research integrating behavioral observations with biomarkers of stress, inflammation, and neurological function could enhance interpretation accuracy. Barbeau et al. (2019) [42] have begun this work by correlating heart rate characteristics with inflammatory markers with hypoxic-ischemic encephalopathy, but more comprehensive models are needed.
Machine learning applications: Artificial intelligence techniques hold promise for identifying subtle communication patterns. Several studies [43-44] have attempted to develop algorithms capable of distinguishing pain-related cries or assessing pain through facial expressions. However, this field is still in its early stages and requires further research.
The interpretation of neonatal communication represents a sophisticated clinical skill that bridges physiological understanding with behavioral observation. This review has demonstrated that neonates, far from being passive recipients of care, actively communicate their needs, preferences, and responses to interventions through an intricate system of behavioral and physiological signals. When properly interpreted, these communication patterns provide invaluable guidance for clinical decision-making and individualized care.
Neonatal communication occurs through multiple intersecting channels—vocalization, body language, facial expressions, and autonomic indicators—each providing complementary information about the infant’s state. The evidence presented throughout this review highlights how structured observation techniques and validated assessment tools significantly enhance clinicians’ ability to accurately interpret these communication signals, particularly when integrated with physiological monitoring. Parents naturally develop specialized expertise in recognizing their infant’s unique communication patterns, making them essential partners in interpreting and responding to neonatal signals.
By recognizing neonates as active communicators and developing the skills to interpret their signals accurately, clinicians and parents can provide care that not only addresses immediate needs but also supports optimal neurodevelopment. This approach transforms neonatal care from a primarily task-oriented practice to a relationship-based model that honors the neonate’s capacity for meaningful interaction and self-regulation.