-
Email info@annpnc.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
Universidade de São Paulo, Faculdade de Medicina de Bauru, Brazil.
*Corresponding author: Lucas Casagrande Passoni Lopes
Universidade de São Paulo, Faculdade de Medicina de
Bauru, Alameda Doutor Octávio Pinheiro Brisolla, 9-75, Bauru – SP, 17012-901, Brazil.
Email ID: lucaspassoni@usp.br
Received: Mar 17, 2025
Accepted: Apr 11, 2025
Published Online: Apr 18, 2025
Journal: Annals of Pediatrics and Neonatal Care
Copyright: Passoni Lopes LC et al. © All rights are reserved
Citation: Passoni Lopes LC. Gut microbiota impact under necrotizing enterocolitis: An overview. Ann Pediatr Neonatal Care. 2025; 1(1): 1003.
Necrotizing Enterocolitis (NEC) is a life-threatening gastrointestinal disease predominantly affecting preterm infants. The pathogenesis of NEC is strongly linked to gut microbiota dysbiosis, characterized by a reduction in beneficial commensal bacteria, such as Bifidobacterium and Lactobacillus, and an increase in pro-inflammatory taxa, particularly Proteobacteria and Clostridium butyricum. This microbial imbalance disrupts intestinal homeostasis, triggers exaggerated immune responses, and compromises the epithelial barrier, contributing to NEC development. Factors such as prematurity, formula feeding, antibiotic exposure, and genetic predisposition further exacerbate microbiota alterations. Specific bacterial species, including Klebsiella oxytoca, Citrobacter, and Enterococcus faecalis, have been implicated in NEC pathophysiology through the activation of inflammatory pathways, such as Toll-Like Receptor 4 (TLR4) signaling, and the production of cytotoxic metabolites. Histopathological changes, including mucosal necrosis, epithelial apoptosis, and impaired regenerative capacity, underscore the devastating impact of dysbiosis on gut integrity. Emerging research highlights the potential of microbiome-targeted interventions, including probiotics, prebiotics, and postbiotics, in restoring gut homeostasis and reducing NEC risk. Advances in metagenomics, metabolomics, and artificial intelligence-driven predictive modeling are expected to revolutionize NEC diagnostics and personalized microbiota-based therapies. This review provides an analysis of the intricate relationship between gut microbiota and NEC pathogenesis, emphasizing the critical need for translational research to optimize neonatal care and improve long-term outcomes.
Necrotizing Enterocolitis (NEC) is a severe gastrointestinal disorder primarily affecting neonates, particularly preterm infants [1]. Characterized by intestinal inflammation, ischemia, and necrosis, NEC can lead to perforation, peritonitis, and multiorgan failure [1]. The condition presents with a broad spectrum of clinical manifestations, ranging from mild feeding intolerance to life-threatening sepsis [1]. Despite advancements in neonatal care, NEC remains one of the most devastating and enigmatic diseases in neonatology, with high morbidity and mortality rates [1].
Epidemiologically, NEC predominantly affects preterm infants, particularly those born before 32 weeks of gestation or weighing less than 1500 grams [2]. The incidence varies depending on gestational age and birth weight, with estimates suggesting that approximately 7-10% of very low birth weight infants develop NEC [2]. The condition imposes a significant socioeconomic burden, leading to prolonged hospital stays, increased healthcare costs, and long-term neurodevelopmental impairments [2]. In severe cases requiring surgical intervention, the financial and emotional toll on families and healthcare systems is profound [2].
Several risk factors contribute to NEC development, including prematurity, formula feeding, hypoxia, hemodynamic instability, and genetic predisposition [3]. However, emerging evidence underscores the pivotal role of the gut microbiota in NEC pathogenesis [3]. Dysbiosis, characterized by an imbalance in intestinal microbial composition, has been implicated in triggering an exaggerated inflammatory response, compromising gut integrity, and facilitating bacterial translocation [3]. Understanding the interplay between microbial communities and host immune responses is essential to elucidate NEC’s underlying mechanisms [3].
Numerous studies have explored the molecular and cellular pathways by which microbiota influences NEC development, shedding light on immune modulation, barrier function disruption, and metabolic interactions [4]. Given the increasing recognition of microbiota’s role in NEC pathophysiology, this brief overreview aims to provide a comprehensive overview of the mechanisms through which gut microbiota impacts NEC onset and progression. By synthesizing current knowledge, this article seeks to enhance our understanding of potential preventive and therapeutic strategies targeting microbiota-related pathways in NEC management.
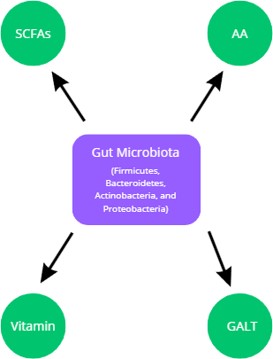
The gut microbiota is a complex and dynamic community of microorganisms that plays a crucial role in maintaining homeostasis within the human body. In a healthy state, the intestinal microbiota consists of a diverse range of bacteria, archaea, fungi, and viruses, with bacterial populations being the most studied [5]. The dominant phyla in the gut microbiota include Firmicutes, Bacteroidetes, Actinobacteria, and Proteobacteria, with specific genera such as Bifidobacterium, Lactobacillus, Bacteroides, and Clostridium playing pivotal roles. These microorganisms contribute to various physiological processes, including digestion, immune modulation, and protection against pathogens [5]. They achieve this by fermenting dietary fibers into Short-Chain Fatty Acids (SCFAs) such as acetate, propionate, and butyrate, which serve as essential energy sources for colonocytes and contribute to intestinal barrier integrity [5]. Additionally, commensal bacteria metabolize amino acids, synthesize vitamins (such as vitamin K and certain B vitamins), and influence the host’s immune system by interacting with Gut-Associated Lymphoid Tissue (GALT), thus promoting immune tolerance and defense against infections [5].
Beyond their metabolic contributions, the gut microbiota engages in a dynamic interplay with host physiology by modulating hormone production, neurotransmitter signaling, and systemic inflammatory responses [6]. Beneficial bacteria such as Bifidobacterium and Lactobacillus are known for their ability to produce antimicrobial peptides and compete with pathogenic microbes for adhesion sites, thereby preventing colonization by opportunistic pathogens [6]. Moreover, SCFAs generated by bacterial fermentation help maintain a balanced pH in the gut, inhibiting the overgrowth of potentially harmful bacteria such as Enterobacteriaceae [6]. These biochemical processes collectively preserve intestinal homeostasis and play a crucial role in neonatal gut development, particularly in preterm infants, whose microbiota composition is more susceptible to environmental perturbations [6]. Figure 1 summarizes these mechanisms.
Despite the resilience of the gut microbiota, numerous genetic and environmental factors can perturb its delicate equilibrium, leading to dysbiosis—a state characterized by reduced microbial diversity and an imbalance between beneficial and pathogenic bacteria [7]. Genetic predisposition plays a significant role in determining an individual’s microbial composition, as host genes influence mucosal immunity, gut motility, and epithelial barrier function [7]. Infants born via cesarean section, for example, exhibit a microbiota composition distinct from those delivered vaginally, with a delayed colonization of beneficial microbes such as Bifidobacterium and an increased prevalence of opportunistic pathogens like Enterococcus and Staphylococcus [7]. Similarly, preterm birth disrupts the natural succession of microbial colonization, resulting in reduced microbial diversity and an increased susceptibility to gut-related disorders such as Necrotizing Enterocolitis (NEC) [7].
Environmental factors such as antibiotic exposure, formula feeding, and Neonatal Intensive Care Unit (NICU) hospitalization further exacerbate microbial imbalances [8]. Antibiotics, while essential for combating infections, indiscriminately eliminate both beneficial and pathogenic bacteria, leading to a loss of microbial diversity and a subsequent overgrowth of facultative anaerobes like Proteobacteria [8]. This shift is particularly concerning in preterm infants, as an overabundance of Proteobacteria has been strongly associated with NEC pathogenesis [8]. Additionally, deviations in microbial metabolites, such as a decrease in SCFAs and an increase in proteolytic fermentation byproducts like ammonia and hydrogen sulfide, contribute to gut inflammation and epithelial damage [8]. These metabolic alterations activate inflammatory pathways, including Toll-Like Receptor 4 (TLR4) signaling, which exacerbates intestinal injury and compromises barrier integrity, creating a favorable environment for NEC development [8].
Microbial species and NEC susceptibility
Several bacterial taxa have been implicated in the development of NEC, with distinct microbial signatures observed in affected neonates [9]. Studies have shown that infants with NEC exhibit an increased abundance of Gammaproteobacteria, particularly Escherichia, Klebsiella, and Enterobacter species, alongside a depletion of protective anaerobes such as Bifidobacterium and Lactobacillus. Klebsiella species, including Klebsiella oxytoca and Klebsiella pneumoniae, have been identified as dominant strains in NEC-aflicted neonates, often replacing Escherichia coli and coexisting with Enterococcus faecalis [9]. Additionally, Clostridium butyricum has been associated with NEC due to its ability to produce cytotoxins that exacerbate intestinal damage [9]. Early microbial colonization patterns also play a crucial role, as the presence of Bacteroides dorei and Clostridium perfringens in the meconium has been linked to an increased risk of NEC, suggesting that initial gut colonization events may predispose infants to disease onset [9].
Biochemical pathways and cytokine activation
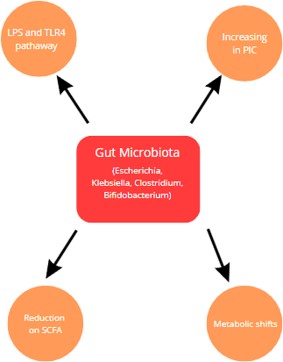
Dysbiosis in NEC is accompanied by significant alterations in biochemical pathways and inflammatory signaling cascades [10,11]. The predominance of Proteobacteria in NEC-aflicted infants correlates with heightened Lipopolysaccharide (LPS) production, which triggers TLR4 activation on intestinal epithelial cells [10]. This activation leads to the release of pro-inflammatory cytokines such as Interleukin-8 (IL-8), Tumor Necrosis Factor-Alpha (TNF-α), and Interleukin-6 (IL-6), which collectively exacerbate gut inflammation and tissue damage [11]. The loss of commensal anaerobes further impairs intestinal barrier function by reducing SCFA production, thereby weakening epithelial tight junctions and promoting bacterial translocation into the systemic circulation [10,11]. Additionally, dysbiosis-induced metabolic shifts favor proteolytic fermentation over carbohydrate fermentation, leading to an accumulation of harmful metabolites such as branched-chain fatty acids and ammonia, which further contribute to mucosal injury and intestinal dysmotility [10,11].
Histopathological and physiological alterations
The pathophysiological consequences of NEC extend beyond microbial imbalances, encompassing severe histo-anatomical and functional alterations [12,13]. Affected neonates exhibit extensive mucosal necrosis, submucosal edema, and transmural inflammation, often leading to perforation and peritonitis [12]. Histological analyses of NEC-affected tissues reveal increased neutrophilic infiltration, crypt abscess formation, and villous atrophy, indicative of severe epithelial disruption [12]. Furthermore, vascular endothelial damage contributes to ischemia and hypoxic injury, exacerbating intestinal necrosis [12]. Physiologically, NEC disrupts gut motility, nutrient absorption, and systemic immune homeostasis, leading to severe metabolic derangements and multi-organ dysfunction [13]. These changes significantly impact the natural history of the disease, with severe cases requiring surgical intervention, including bowel resection, which may result in short bowel syndrome and longterm nutritional challenges [13].
Impact on disease progression and prognosis
NEC remains a leading cause of morbidity and mortality in preterm infants, with outcomes largely dictated by disease severity and the extent of intestinal involvement [14,15]. The disruption of gut microbiota early in life has long-term consequences, including an increased risk of neurodevelopmental impairments due to gut–brain axis dysregulation [14]. Emerging evidence suggests that NEC survivors exhibit altered metabolic profiles, increased susceptibility to inflammatory disorders, and an elevated risk of sepsis due to persistent microbial imbalances [15]. Probiotic interventions aimed at restoring microbial homeostasis have shown promise in mitigating NEC risk, with strains such as Bifidobacterium longum subsp. Infants demonstrating protective effects by enhancing gut barrier integrity and modulating immune responses [14,15]. However, further research is needed to refine microbiome-targeted therapies and optimize their efficacy in preventing NEC in high-risk populations figure 2 summarizes the mechanisms previously described in this and others text sections [14,15].
The study of gut microbiota in NEC remains an evolving field, with emerging research highlighting novel diagnostic, preventive, and therapeutic approaches [16,17]. Advances in multiomics technologies, including metagenomics, transcriptomics, and metabolomics, are enabling a more comprehensive understanding of microbial composition, metabolic pathways, and host-microbe interactions in NEC [16,17]. Future studies are expected to focus on personalized microbiome-based interventions, leveraging artificial intelligence and machine learning to predict NEC risk and tailor probiotic and prebiotic therapies [16]. Additionally, the role of virome and fungal communities in gut dysbiosis warrants further investigation, as recent findings suggest that bacteriophage-host dynamics may influence microbial resilience. Immunomodulatory strategies targeting the gut-immune axis, such as engineered probiotics and Fecal Microbiota Transplantation (FMT), hold promise in restoring gut homeostasis in vulnerable neonates [17]. Expanding clinical trials on microbiota-based therapies and their long-term impact on neurodevelopmental outcomes will be crucial in translating these insights into effective NEC prevention and management strategies [16,17].
Necrotizing enterocolitis (NEC) represents a severe neonatal condition with significant morbidity and mortality, closely linked to alterations in gut microbiota composition. A growing body of evidence suggests that dysbiosis, characterized by an overrepresentation of pro-inflammatory bacterial taxa and a reduction in beneficial commensals, contributes to disease pathogenesis through immune dysregulation and intestinal barrier compromise. Understanding the intricate microbial-host interactions and the biochemical pathways involved provides valuable insights into novel preventative and therapeutic strategies. The ongoing advancement of microbiome research, coupled with emerging technological innovations, offers a promising avenue for mitigating NEC burden and improving neonatal health outcomes.